"A partial or full tear of the ulnar collateral ligament represents a structural failure under extreme valgus torque. Reconstructing this stabilizing bridge requires a meticulous progression from mechanical protection to dynamic, sport-specific energy transfer."
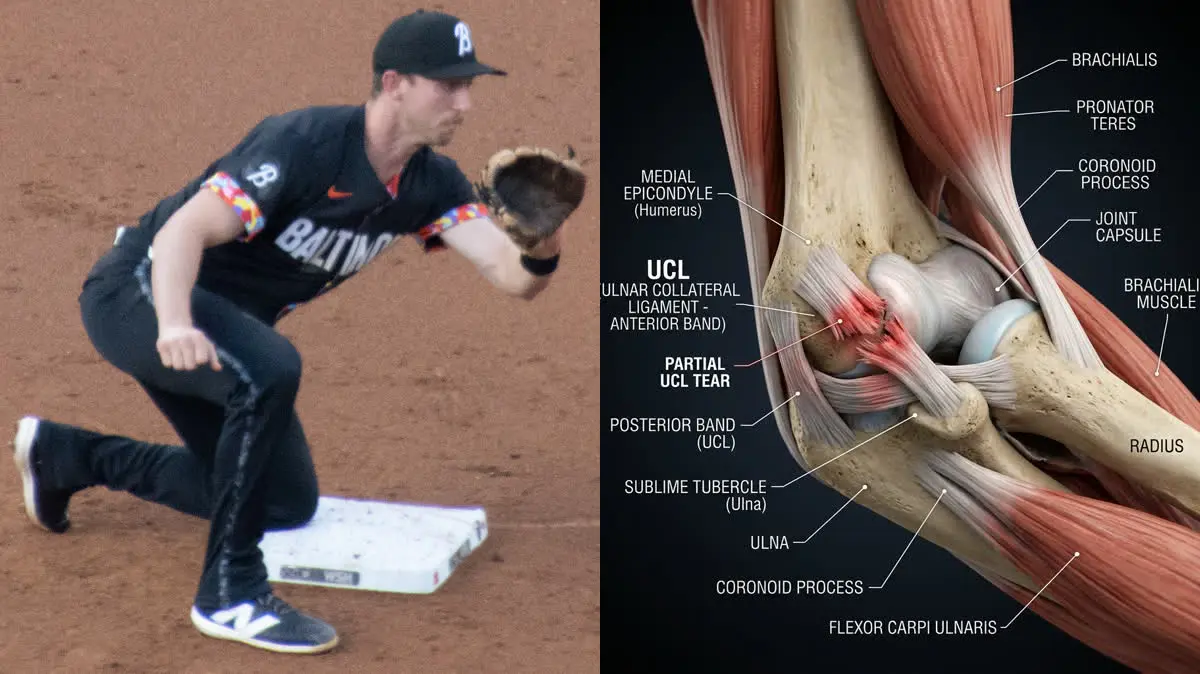
In May 2026, the Baltimore Orioles faced a significant setback with the announcement that their standout infielder, Jordan Westburg, would undergo season-ending Tommy John surgery. The procedure aims to repair a partial tear of the ulnar collateral ligament (UCL) in his right elbow, closing the door on his promising 2026 campaign. While Tommy John surgery is a well-established route for pitchers, Westburg's injury underscores that position players are also highly vulnerable to the repetitive, high-velocity throw loads that compromise medial elbow stability.
The road back from a UCL reconstruction is long and demanding. In this clinical biomechanical analysis, we will explore the anatomy of the UCL, examine the extreme forces that cause tears, explain the surgical grafting techniques, and detail the four main phases of the physical therapy rehabilitation protocol.
The Anatomy of the Medial Elbow: The UCL Complex
The elbow is a hinge joint that relies heavily on both bony congruence and ligamentous constraints to maintain alignment under load. The primary stabilizer against valgus stress (forces pushing the elbow inward and the forearm outward) is the ulnar collateral ligament (UCL), located on the medial side of the joint. The UCL complex consists of three distinct bands:
- The Anterior Band: This is the strongest and most functionally significant component of the UCL. It spans from the medial epicondyle of the humerus to the sublime tubercle of the ulna. It acts as the primary constraint against valgus force throughout the entire range of elbow flexion.
- The Posterior Band: This fan-shaped band stabilizes the joint primarily at higher angles of flexion (beyond 90 degrees) but plays a secondary role compared to the anterior band.
- The Transverse Band: This band connects the ulna to itself and contributes minimally to overall joint stability.
During the throwing motion, the anterior band of the UCL is subjected to tension forces that closely approach its ultimate tensile strength, leaving very little margin for error. Over time, repetitive throwing leads to microtrauma, laxity, and eventually, a structural tear.
- During a high-velocity throw, the elbow experiences a valgus torque of up to 64 Newton-meters (Nm), which is equivalent to hanging a 60-pound weight from the hand.
- The UCL itself absorbs approximately 54% of this total valgus stress, with the surrounding muscles (pronator teres, flexor carpi ulnaris) absorbing the rest.
- Tommy John surgery (UCL reconstruction) has a successful return-to-play rate of 80% to 90% in professional baseball players.
- The average recovery time for position players returning to competitive game action is 9 to 12 months, compared to 12 to 18 months for pitchers.
Biomechanical Triggers: The Physics of the Throw
The biomechanics of throwing can be divided into several phases: wind-up, stride, cocking, acceleration, deceleration, and follow-through. The highest risk to the UCL occurs during the late cocking and early acceleration phases. During late cocking, the shoulder is in maximum external rotation and the elbow is flexed at approximately 90 degrees. This positioning subjects the medial elbow to massive valgus torque.
If the kinetic chain is disrupted—such as by weak hip stabilizers or poor core transfer—the thrower will compensate by using the arm to generate velocity. This "arm throwing" increases the valgus load on the medial elbow, overloading the anterior band of the UCL. In position players, quick, off-balance throws from the infield under high-pressure situations can trigger acute tears when the body is out of alignment.
"In position players like Jordan Westburg, returning to play requires more than just waiting for the reconstructed ligament graft to heal. The graft (often harvested from the palmaris longus tendon in the forearm or a hamstring tendon) must undergo a process called ligamentization, where the tendon slowly transforms into a functional ligament. Rushing the throwing program before this cellular reorganization is complete leads to graft elongation, laxity, and eventual failure."
The UCL Reconstruction (Tommy John) Rehabilitation Protocol
Rehabilitation after Tommy John surgery is a highly structured, criteria-based progression designed to protect the graft while restoring complete range of motion and muscular strength.
- 1Phase 1: Graft Protection and Early Range of Motion (Weeks 1–4)The elbow is immobilized in a hinged brace, initially locked at 90 degrees. Passive range of motion is gradually introduced, progressing from 30 to 100 degrees by week 2, and 15 to 110 degrees by week 4. Hand grip exercises and shoulder/wrist isometrics are performed daily to prevent muscle atrophy without placing valgus stress on the elbow.
- 2Phase 2: Progressive Strengthening and Full ROM (Weeks 5–8)The goal is to achieve full elbow extension and flexion by week 8. The brace is discontinued for daily activities. Light active-assisted and active exercises are introduced, including wrist curls, elbow flexion/extension, and forearm pronation/supination. Strengthening of the rotator cuff, scapular stabilizers, and core is emphasized.
- 3Phase 3: Advanced Conditioning and Plyometrics (Weeks 9–16)Eccentric strengthening of the forearm flexor-pronator mass is introduced, as these muscles act as dynamic stabilizers of the medial elbow. Light plyometric drills (two-handed medicine ball throws) begin. Focus is placed on correcting kinetic chain deficits in the hips and thoracic spine to prepare the athlete for throwing.
- 4Phase 4: Interval Throwing Program (Weeks 17+)Once the athlete is pain-free and has passed a comprehensive biomechanical screening, a structured interval throwing program begins. Throwing starts on flat ground at short distances (30–45 feet) with a high arc, gradually increasing intensity and distance. Position players transition to throwing from their specific infield positions before returning to full competitive play.
The Patient: Tyler, a 21-year-old shortstop who sustained a partial UCL tear and underwent Tommy John reconstruction.
The Mistake: Tyler attempted to skip the early phases of scapular and core stability training, focusing solely on elbow strength. When he began throwing, he experienced recurring medial joint pain due to poor scapular control.
The Solution: We paused his throwing program and spent 4 weeks correcting his scapulohumeral rhythm, strengthening his lower trapezius, and improving his hip-rotation mobility.
The Outcome: Tyler resumed his throwing program pain-free and returned to competitive play 10 months post-surgery, with improved throwing velocity and zero elbow discomfort.
Systemic Kinetic Health: The Broader View
Elbow stability is intimately connected to the health of the entire upper extremity. To understand how the shoulder interacts with the arm, read our guide on rotator cuff tendinopathy and eccentric strengthening. If you are managing chronic shoulder tightness that limits your throwing mechanics, study our analysis of scapulohumeral rhythm in shoulder impingement. Additionally, for athletes recovering from other major joint reconstructions, our review of the best post-operative knee braces offers vital insights into joint bracing strategies.
Jordan Westburg's road to recovery will require patience and strict adherence to his rehabilitation protocol. By focusing on total-body biomechanics, strengthening the dynamic muscle stabilizers of the forearm, and allowing the graft to mature fully, he can return to the Orioles' lineup with his throwing arm stronger and more resilient than ever. Tommy John surgery is a grueling process, but it remains a reliable path for elite athletes to reclaim their careers and return to the highest level of sport.
Featured image: Clinical side-by-side composite showing Jordan Westburg in action (left) and an anatomical 3D rendering of an elbow joint with a partially torn ulnar collateral ligament (right). Created for AyurPhysio editorial use. Wikimedia Commons attribution: Jordan Westburg image by Keith Allison licensed under CC BY-SA 2.0. Modified by cropping and compositing.
Dr. Dhanushika Dilshani
Expert Ayurvedic Wellness Doctor. Specialized in modern holistic wellness, optimizing dermal resilience, cosmetic radiance, and systematic diagnosis driven by traditional and evidence-based medical logic.
Medical Disclaimer
The information provided by AyurPhysio is for general educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Related Healing Guides
View All Guides →
Christian Eriksen's Cardiac Arrest and ICD Return to Play: The Biomechanics of Cardiorespiratory Reconditioning and Athletic Heart Rehabilitation

Selena Gomez's Lupus and Kidney Transplant: An Integrative Ayurvedic Approach to Systemic Autoimmunity, Dushi Visha, and Ojas Restoration
